Brain and spine tumors are one of the most common forms of cancer found in kids, second only to leukemia. Despite significant advances in treatment, brain tumors remain the leading cause of cancer-related death in children. The kids who do survive often suffer from long-term side effects from treatment, and face the risk of recurrence or developing a secondary cancer.
Recent advances in technology have resulted in improved diagnosis and classification of brain tumors. Often, tumors that appear to be similar under a microscope and would have previously been considered the same type of cancer are now understood to be distinct at a molecular level, have varying prognoses, and respond differently to treatment.
To give kids with cancer the best chance at long-term survival, treatment cannot be a “one size fits all” approach. A strategy must be individualized to the child’s specific type of cancer to increase the effectiveness of treatment, reduce complications, and improve overall survival rates. And to do that, better models that mimic how the tumor forms and grows and predict response to treatment are vital.
Pediatric brain tumor models are categorized into two groups. In vitro means “in glass” in Latin and describes experiments that are performed outside of a living organism, like in a petri dish. Experiments that are performed in a whole living organism are known as in vivo, which is Latin for “within the living”.
Two of the most common and important models for testing treatments for pediatric brain tumors are cancer cell lines and xenograft models.
Cancer cell lines can be established directly from patient samples, which is why a family’s decision to allow their child’s tumor to be used in research is very meaningful. Cancer cells grown from cell lines retain the original features of the tumor, can be easily grown, and can be stored for a long time. Cell lines are very useful in high-throughput drug screening to identify and evaluate potential chemotherapy targets. In vitro cell line models are limited because they cannot replicate the diversity found in tumors or the interaction between the tumor and the environment in which it grows in the body.
Xenograft models are made by transplanting established cancer cell lines or patient tumor tissue into host animals, most often mice for brain tumor research. Tumors can be established in the normal location in the body (orthotopic) or elsewhere (heterotopic). These in vivo models are used to understand the biological mechanisms of brain tumors and their microenvironment for testing new treatments. Because the host animal is immunodeficient, xenograft models cannot account for the contribution of the immune system in the formation and growth of tumors in humans.
Cell lines and xenograft models are both valuable tools for studying and improving treatment options for kids with cancer, but new models are needed to unleash vital information. Researchers need to be able to study cancer in a way that more closely mimics what happens in the body, including how the immune system plays a role in cancer and the ways in which tumors form and grow in three dimensions.
Because of donor support, researchers are working right now to create new models for testing pediatric cancer treatments.
These advanced models will provide a deeper understanding of how cancers form and develop in the brain and spinal cord. They will also allow for better testing of new treatment ideas so that viable options can get to kids with cancer who desperately need them as quickly as possible.
Here’s a look at just a few of the models being developed right now:
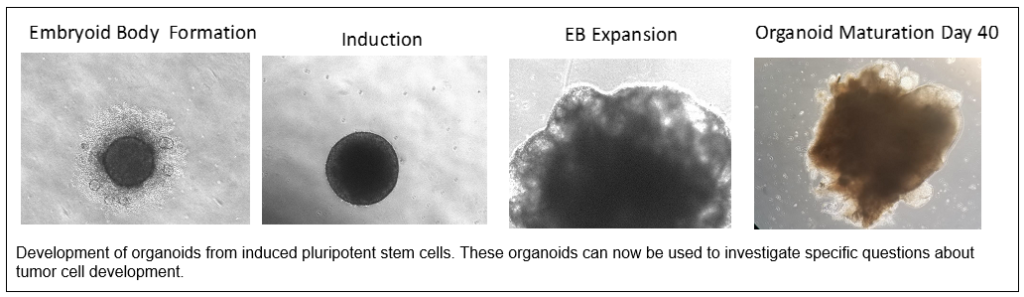
Dr. Rajeev Vibhakar and senior researcher Irina Alimova are using organoids in their work on ATRT, a highly aggressive type of pediatric brain tumor with an overall survival rate of just 35%.
Organoids are an emerging technology where a miniature and simplified version of an organ is created in vitro in three dimensions. Organoids are generated using induced pluripotent stem cells (iPSCs) that can be grown into a 3D architecture that mimics natural tissue development because the cells can self-renew and differentiate into different types of cells.
Dr. Vibhakar’s team is using an organoid model of neural cell development that allows them to evaluate brain and tumor cell development.
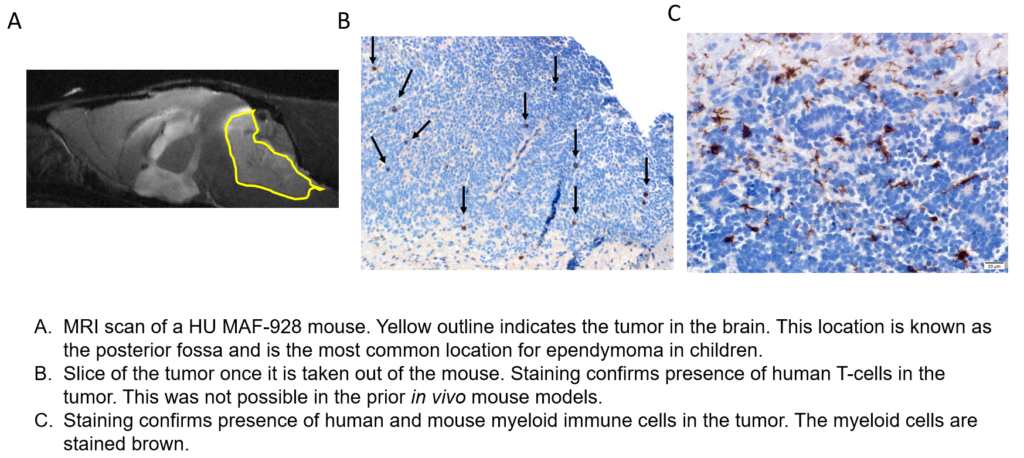
Dr. Nick Foreman and senior researcher Andrea Griesinger are working to develop a new xenograft model that will allow them to evaluate the role of the interaction between the tumor and the immune system in pediatric brain tumors.
To study the tumor/immune system interaction, a model with an intact immune system is needed. This is not possible with in vitro models and is different from most in vivo studies where the mice do not have an immune system to ensure the tumor will grow. So, Dr. Foreman’s team is developing an in vivo humanized immune mouse model.
Two patient-derived ependymoma lines have been created in mice with humanized immune systems. The team is now studying the interaction between the tumor and the immune system in ways not previously possible.
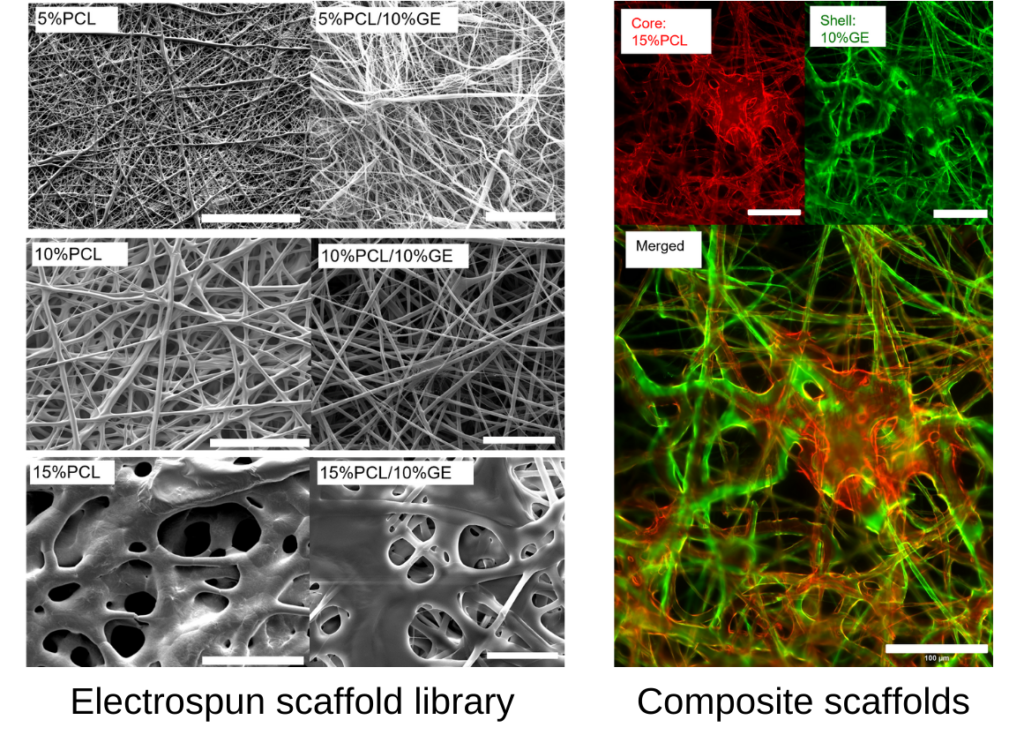
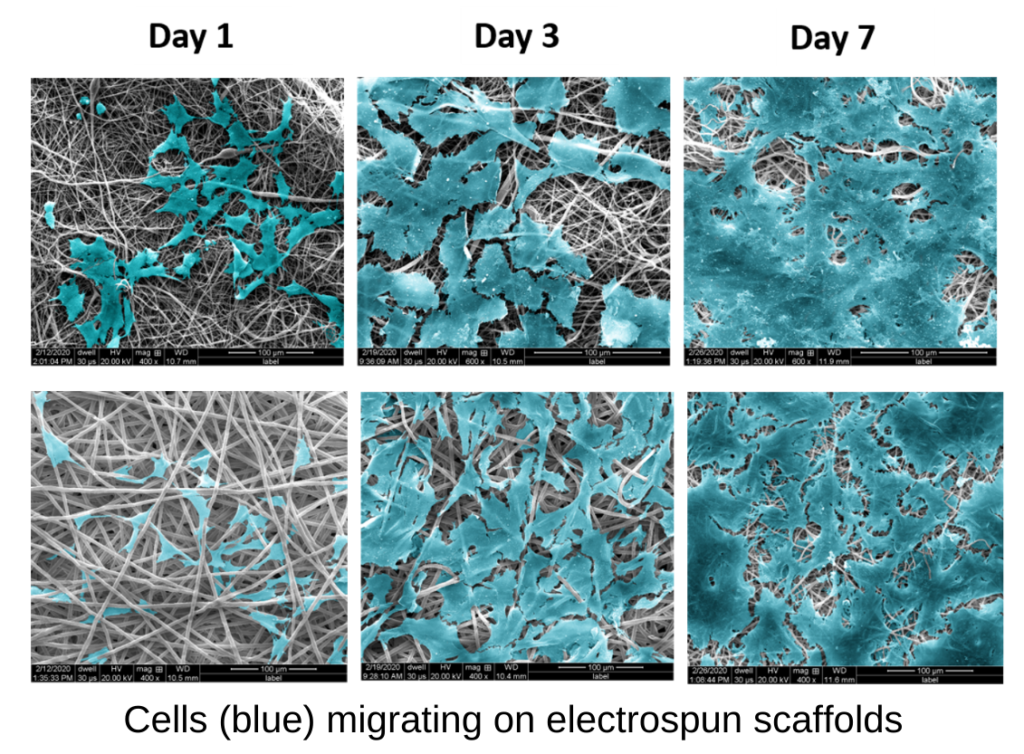
Rachael Sirianni and her team are studying the spread of pediatric brain tumors through the cerebrospinal fluid called leptomeningeal metastasis (LM).
Leptomeningeal metastasis is a devastating complication of many types of pediatric brain tumors, including medulloblastoma, ependymoma, and ATRT. Kids with LM face poor long-term outcomes, so this research is critical.
There is no model to study LM in the laboratory, so Dr. Sirianni’s team is creating a bioengineered in vitro model using polymer scaffolds that mimics the fibrous structure of the leptomeningeal compartment.